
The Agency That Runs the Program, Judges Its Harms, and Controls Its Own Information
Why Korea’s disease control agency was structurally incapable of producing the trust it needed

The Architecture of Distrust — Essay #7
This is the seventh and final essay in The Architecture of Distrust. The series was originally planned as six essays; a seventh was added when the cognitive layer between the science and the institution demanded its own account.
The previous essays described the components: a legal standard that requires only temporal proximity, a court ruling that treated decades of science as an unknown, and — beneath both of these — the cognitive architecture that makes temporal inference feel like evidence. The tools to evaluate causation properly exist. The WHO AEFI algorithm, the Brighton Collaboration case definitions — these were built precisely because the cognitive patterns are known and predictable.
What this essay asks is why the institution responsible for using them could not.
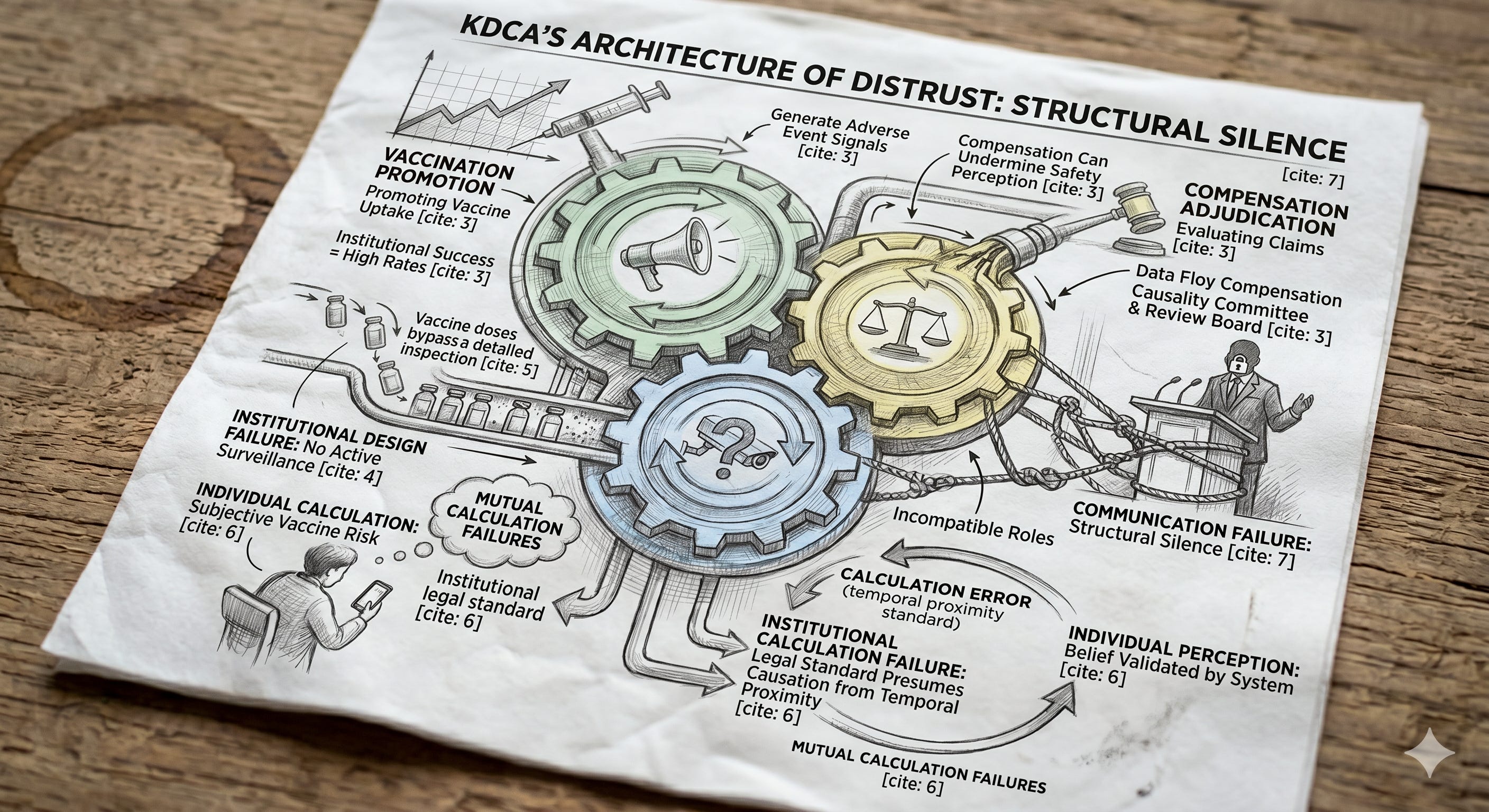
The Korea Disease Control and Prevention Agency (KDCA) occupies a position that, once described, is difficult to see as anything other than a conflict of interest. The agency performs three functions simultaneously.
First, it administers the national vaccination program — procuring vaccines, setting the immunization schedule, coordinating delivery, and promoting uptake. Its institutional success is measured, in part, by vaccination rates. A high rate is evidence of a functioning program. A declining rate is a problem to be managed.
Second, it receives and adjudicates claims for vaccine injury compensation. When a citizen reports an adverse event following immunization, the report enters the KDCA’s system. A causality assessment committee — convened under the agency’s authority — evaluates the claim. A compensation review board — also under the agency’s authority — determines whether payment is warranted.
Third, the KDCA operates Korea’s passive adverse event surveillance system. Reports of adverse events following immunization are submitted to the agency. The agency is the endpoint. It receives the signal, evaluates its meaning, and decides what to communicate about it.
These three functions — promotion, adjudication, and surveillance — sit within the same institution. The agency that encourages citizens to get vaccinated is the same agency that decides whether the vaccine harmed them and the same agency that monitors whether the vaccine is causing harm at all.
This combination is unusual. Most national immunization programs distribute these functions across separate institutions. What makes the Korean case distinctive is not only this combination but what was not built alongside it.
What every national immunization program requires — whatever its institutional arrangement — is post-market pharmacovigilance. This is not a single mechanism but an integrated system. Passive surveillance detects signals from spontaneous reports of adverse events. Active surveillance verifies, at the population level, whether those signals represent real risk — comparing post-vaccination event rates against pre-vaccination or unvaccinated-population baselines. The verified output forms the evidentiary basis for vaccination policy and for the safety information communicated to the public.
When the three administrative roles are concentrated in a single institution, this safety function becomes more critical, not less. It is the function Korea did not build.
What Korea has, formally, is passive surveillance. Adverse event reports flow into the KDCA. But the institutional pathway through which reports are processed is not, in practice, a safety information pathway. It is a compensation pathway. When a report becomes a compensation claim, it enters the Damage Investigation Team, which assesses individual cases; those assessments feed the Compensation Committee, which decides whether individual payment is warranted. The signal exits this pipeline as a compensation determination — not as a population-level safety question.
The active surveillance layer was not absent. It was outsourced. In the years following the COVID-19 vaccination rollout, the KDCA contracted the Korean Academy of Medical Sciences to conduct post-authorization safety studies — the kind of population-level verification work that compares observed against expected incidence. The studies were commissioned. The data was generated. But the epidemiological output did not flow into an independent safety assessment that could be communicated to the public or used as evidence for vaccination policy. It flowed back into the same compensation-decision process — used to determine which conditions, in which patients, would meet the criteria for individual payment.
The result is not “active surveillance is missing.” That is a symptom. The actual structural failure is that post-market pharmacovigilance — as an integrated system that converts surveillance signals into safety information, and safety information into policy and public communication — was never set up. A national immunization program requires this function separately from the drug regulator’s pharmacovigilance role: to inform its own program decisions, to communicate benefit-risk to citizens, and to respond to safety events including the misinformation that often follows serious but coincidental adverse outcomes. The KDCA, running program and compensation simultaneously without this function, produced something else: a system that issues individual compensation decisions while the safety information the public is owed simply disappears.
This is what purpose contamination looks like. Not a single instrument routed to the wrong output, but an entire surveillance architecture reorganized around a different question. A safety assessment asks what is true at the population level. A compensation decision asks what is owed to a particular person. When the institutional pathway that should have produced the first instead produces only the second — and when the institution responsible for that pathway is also responsible for the program whose safety it should be evaluating — the result is not a system that does two things. It is a system that does neither well.
This structure produces a specific kind of failure that is worth naming precisely.
The 7C framework used in vaccine hesitancy research measures readiness along seven dimensions. One of them — Calculation — describes the individual’s subjective assessment of vaccine risks and benefits. When an individual overestimates risk or underestimates benefit, that is a Calculation failure at the individual level.
What Korea’s institutional design produced is something different: a Calculation failure at the institutional level. The legal standard described in the previous essays — “does not appear impossible” — accepts temporal proximity without background rates as sufficient evidence of causation. This is, in epidemiological terms, a Calculation error: it fails to compare observed events against expected events. But this error was not made by a frightened parent scrolling through a social media feed. It was made by a court, codified in legislation, and operationalized by the agency responsible for public health.
The consequence is a feedback loop. When the institution’s own standard of causation embeds a Calculation error — when the law presumes causation from temporal proximity alone — the public’s individual Calculation is not merely uninformed. It is validated by the institution. The parent who believes the vaccine caused their child’s illness is not contradicted by the system. The system agrees. Not because the evidence supports the belief, but because the legal standard does not require evidence.
This is the architecture. Not a single decision, not a single person, not a single failure point — but a structural arrangement in which the agency that should be the most trusted source of vaccine safety information is the agency least capable of producing it, because its own design makes every communication suspect.
By March 24, 2026, only 42.7 percent of Korea’s high-risk population — adults 65 and older, the immunocompromised, and residents of long-term care facilities — had received the 2025–26 seasonal COVID-19 vaccine. The KDCA’s own briefing acknowledged that six in ten of those at highest risk remained unvaccinated.
These are the people for whom the benefit of vaccination most clearly outweighs the risk.
There is a final element, and it concerns what was not said.
During the period covered by this series, the World Health Organization’s Strategic Advisory Group of Experts on Immunization reaffirmed COVID-19 vaccine safety and effectiveness; the U.S. Advisory Committee on Immunization Practices continued to issue recommendations grounded in benefit-risk evaluation. These are the kinds of communications a national vaccination program receives and re-articulates for its own citizens.
The KDCA’s AEFI surveillance data and investigation findings did not enter that flow. They produced no safety messaging. They anchored no policy communication. What did enter the public domain — primarily through National Assembly submissions and parliamentary inquiries — were compensation statistics: the number of vaccine injury claims filed, the number adjudicated, the number rejected. Most of those claims involved temporally coincident events with no demonstrated causal relationship to vaccination. But the public did not receive that distinction. It received a count.
What reached citizens was not “this vaccine is safe.” It was “most claims of vaccine injury have been rejected.” The first message builds confidence. The second, in the absence of any frame for distinguishing coincidence from causation, reads as institutional dismissal — and the more the compensation system publishes, the more it propagates the perception it was meant to dispel.
This was not a failure of will. It was a failure of capacity — and the capacity failure was structural. An agency that adjudicates individual compensation claims has an institutional interest in not making public statements about population-level causation, because those statements could be used against it in court. An agency that promotes vaccination has an institutional interest in not highlighting adverse events. An agency that controls its own information flow has no external pressure to disclose what it has not been asked to disclose.
The result is an agency that cannot speak — not because it does not know, but because its structure makes every possible statement a liability. Safety information, if published, could undermine compensation decisions. Compensation generosity, if highlighted, could undermine vaccination promotion. Surveillance data, if released, could be misinterpreted in the absence of the analytical context that the agency never built.
The gap that the courts filled was not created by judicial overreach. It was created by institutional silence. And the silence was not a choice. It was the inevitable output of a structure that was designed to perform three incompatible functions simultaneously.
Japan silenced the science by making it irrelevant to the decision. Korea produced a different kind of silence — not by overriding the evidence, but by building an institution that could not communicate it without damaging itself.
The architecture is different. The silence is the same.
References
Geiger M, Rees F, Lilleholt L, et al. Measuring the 7Cs of vaccination readiness. Eur J Psychol Assess. 2022;38(4):261-269. doi:10.1027/1015-5759/a000700
Korea Disease Control and Prevention Agency. 고위험군 대상 ‘25-’26절기 코로나19 예방접종 연장 안내 [Extension of 2025–26 Seasonal COVID-19 Vaccination for High-Risk Groups]. Press briefing materials. April 15, 2026. (Reports 42.7% vaccination rate among high-risk groups as of March 24, 2026; references WHO SAGE meeting of March 9–12, 2026 reaffirming COVID-19 vaccine safety and effectiveness.)
Kang CR, Choe YJ, Yoon SJ. COVID-19 Vaccine Injury Compensation Program: Lessons Learned From a Review of 10 Implementing Countries. J Korean Med Sci. 2024;39(13):e121. doi:10.3346/jkms.2024.39.e121
Chu K, Kim K, Yang J, et al. Analysis of the COVID-19 Vaccine Injury Compensation Program in Korea. Vaccine. 2025;47(3):126726. doi:10.1016/j.vaccine.2025.126726